You may be doing this search late at night, between work emails, after a difficult conversation at home, or after one more promise to yourself that things will be different tomorrow. For professionals and executives, the first problem usually isn't finding a program. It's sorting through a crowded market without exposing private details, derailing work obligations, or walking into a facility that sounds polished but lacks real clinical depth.
Costa Mesa can make that harder and easier at the same time. There are a lot of options, which means access is strong, but it also means families have to separate good care from good marketing. If you're looking for a Costa Mesa CA rehab, the practical questions matter more than the brochure language. Can you detox safely? Can the program treat anxiety, depression, trauma, or burnout at the same time? Will you be allowed enough privacy and limited work access to commit to treatment? And what will insurance cover once the executive label is stripped away?
The families I've seen make the best decisions don't start by asking which center looks nicest. They start by asking which setting matches the medical risk, the psychiatric picture, the level of privacy needed, and their financial plan. That approach cuts through a lot of noise.
Starting the Search for Rehab in Costa Mesa
At 11 p.m., this search often feels less like research and more like risk management. A spouse is asking whether treatment can start this week. An executive is asking whether anyone at work has to know. Someone else is privately wondering how much this will cost if insurance approves only part of the stay.
That is why the first pass should be practical. Costa Mesa has enough treatment options that families can lose days comparing websites, touring attractive houses, and hearing polished admissions calls without getting a clear answer on clinical fit, privacy, or cost. For professionals, those three issues usually decide whether treatment is realistic.
Start by narrowing the field with a Costa Mesa addiction treatment resource, then verify details directly with each program. Use the website to build a shortlist. Use the call to test whether the facility can answer hard questions clearly.
Start with these four screening questions
What are you paying for, and what is extra?
Ask for a plain explanation of what the daily rate includes. Confirm whether detox, psychiatry, medications, lab work, family sessions, transportation, and aftercare planning are billed separately. Executive-focused programs sometimes advertise privacy and work accommodations, but those features may raise the private-pay cost.How private is the setting in practice?
Privacy means more than a nice room. Ask about census size, private or shared bedrooms, visitor policies, phone access, staff handling of professional identity, and whether the program is used to working with physicians, attorneys, founders, or public-facing clients. A facility should explain its confidentiality procedures without sounding evasive.Who decides whether insurance is enough?
Many families hear that a center "takes insurance" and assume the stay is covered. That is rarely the full story. Ask what level of care the insurer is likely to authorize, how often reviews happen, what happens if coverage ends early, and what the private-pay rate becomes after benefits are exhausted.Can the person realistically step away from work?
Some professionals do better with no device access for an initial period because divided attention keeps treatment shallow. Others have legal, operational, or fiduciary duties that require limited contact. The right program sets boundaries that protect treatment, not a fantasy schedule that keeps the person half at work and half in care.
One sentence matters early. "What kind of client are you set up to treat well, and what usually makes someone a poor fit for your program?"
Strong admissions teams answer that directly. They can explain cost trade-offs, privacy limits, and whether the facility can support a professional who needs discretion without promising special treatment that interferes with recovery. Weak teams usually drift back to amenities or avoid specifics about money.
Families make better decisions when they compare programs on fit, privacy, and financial clarity before they compare atmosphere. That approach saves time, reduces surprises, and makes the next call more productive.
Understanding the Levels of Care Available
A common admissions mistake happens on the first call. A spouse says, "He can do evenings, but he cannot disappear for 30 days," or an executive says, "I only need detox." Sometimes that works. Often it puts the person in a level of care that fits the calendar better than the clinical picture.
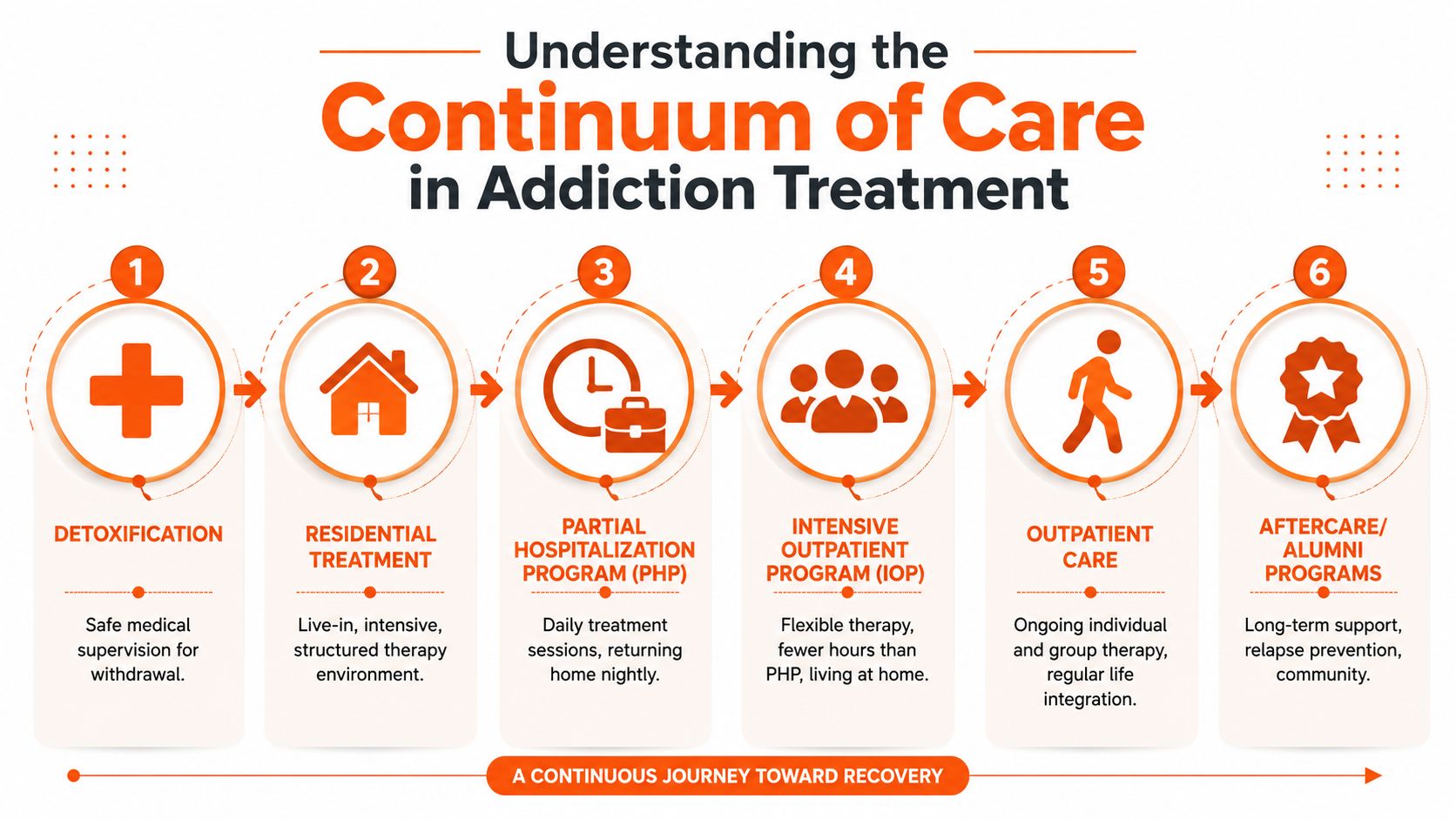
"Rehab" is not one service. It is a sequence of settings with different levels of medical oversight, structure, and freedom. The right question is simple: where can this person stay safe, engage honestly, and keep going after the immediate crisis settles?
A practical overview of the different levels of care in rehab helps families compare programs based on function, not marketing labels.
Detox and residential treatment
Medical detox is the front end of treatment for people at risk during withdrawal from alcohol, benzodiazepines, opioids, or other substances that can cause significant medical or psychiatric complications. Detox focuses on stabilization. Staff monitor symptoms, manage medications, and address urgent issues such as dehydration, blood pressure changes, sleep disruption, or confusion.
Families often expect detox to produce insight or commitment. It usually does not. It gets the person medically and mentally steady enough to start actual treatment.
Residential treatment adds time, structure, and distance from the routines that support substance use. Clients live onsite, follow a full clinical schedule, and have less access to the people, places, and work patterns tied to relapse. For professionals and executives, that separation can feel expensive in every sense. Income may pause. Privacy concerns go up. So does resistance. But if the person cannot stay sober at home, keeps leaving outpatient early, or needs close observation, residential care often saves money compared with repeated failed starts.
PHP, IOP, outpatient, and aftercare
Step-down care matters just as much as the first placement. A strong discharge plan should already be taking shape while the person is still in treatment.
Here is the practical difference between the main options:
Partial Hospitalization Program (PHP)
PHP provides a full day of treatment with substantial clinical contact, while the client sleeps at home or in sober housing. It fits people who need a high level of support but do not require overnight medical supervision.Intensive Outpatient Program (IOP)
IOP offers fewer treatment hours than PHP and more room for real-life responsibilities. This level can work well for someone returning to work in a limited way, provided home life is stable and the program sets clear boundaries around availability.Outpatient therapy
Standard outpatient care usually means individual therapy, group therapy, medication management, or a mix of those services on a lighter schedule. It works best for people with solid follow-through, lower relapse risk, and a recovery environment that is actually supportive.Aftercare and recovery support
Aftercare may include alumni programming, ongoing therapy, peer support, relapse planning, and psychiatric follow-up. Without that structure, discharge turns into a vulnerable gap instead of a planned transition.
For families comparing Costa Mesa programs, the trade-off is usually not luxury versus basic care. It is structure versus flexibility, and cost today versus the cost of relapse later. A high-functioning professional may look appropriate for outpatient care because they can still answer email, attend meetings, or keep up appearances. That can be misleading. The more useful measure is whether they can tolerate reduced control, accept treatment intensity, and remain accountable when no one is watching.
A sound placement decision matches the person to the level of care they can complete, not the one they find easiest to accept on day one.
Evaluating Clinical Quality and Dual Diagnosis Care
A polished website doesn't tell you much about clinical quality. The issue is whether the program can treat the addiction and the condition underneath it at the same time. For executives and professionals, that often includes stress injuries from long-term overperformance, unresolved trauma, depression masked by achievement, or anxiety that people have normalized for years.
What evidence-based care looks like in practice
Facilities often list therapies like CBT, DBT, and EMDR. Those names matter, but the bigger question is how they're used. Evidence-based care isn't just having the acronym on a webpage. It means clinicians use those approaches purposefully, at the right time, with the right patient.
- CBT helps identify and change thought patterns that fuel substance use.
- DBT is useful when emotional regulation, distress tolerance, or impulsive behavior drives relapse.
- EMDR may be appropriate when trauma is part of the story and the patient is stable enough to process it.
Clinical timing matters. In executive rehab settings, medical detox with 24/7 nursing and psychiatric oversight is critical because it reduces acute physiological stress and allows earlier use of psychotherapies such as CBT, DBT, and EMDR, as explained in Beginnings Treatment's executive addiction treatment overview. That's the difference between a medically grounded program and one that treats detox like a formality.
Dual diagnosis is not an add-on
If a program says it treats dual diagnosis, ask what that means operationally. The answer should include psychiatric evaluation, medication management when appropriate, and communication between the addiction team and mental health providers. If those pieces are fragmented, the patient often gets mixed messages.
For many professionals, the substance use problem isn't separate from the mental health problem. Drinking may be managing panic. Stimulant misuse may be tied to untreated ADHD or pressure to perform. Sedatives may be masking insomnia and trauma. Treating only the substance use leaves the main driver untouched.
A useful benchmark is whether the program can describe the patient's care in an integrated way, not as two parallel tracks.
If the admissions team can explain detox in detail but gets vague when you ask about psychiatry, trauma treatment, or medication stabilization, keep looking.
Questions worth asking on the first call
Ask direct questions and listen for direct answers:
| Question | Strong answer sounds like |
|---|---|
| Who evaluates mental health needs? | A psychiatrist or qualified psychiatric provider is part of care |
| How is medication handled? | The program monitors, adjusts, and coordinates medications thoughtfully |
| When do trauma therapies begin? | Only after stabilization and clinical readiness |
| How often does the team review the plan? | Regular interdisciplinary review, not a one-time intake note |
If you want a concrete example of what integrated care should address, this overview of dual diagnosis treatment for executives captures the standard professionals should expect. The key is simple. Don't settle for a program that can talk about addiction but not the person living with it.
Specialized Features for Executives and Professionals
Traditional rehab models don't work for every professional. Some programs treat all outside contact as a threat to recovery. For some clients, that's appropriate. For others, it becomes the reason they delay treatment altogether. A business owner may need to approve payroll. A physician may need to coordinate a leave. An attorney may need to hand off urgent matters confidentially. These aren't lifestyle preferences. They're barriers that can keep someone from entering care.
Standard residential care versus executive-focused care
The biggest difference is design. Standard programs often rely more heavily on groups, shared rooms, fixed communication restrictions, and larger populations. Executive-focused settings tend to build around privacy, individualized care, and controlled connectivity.
Here's the side-by-side trade-off:
| Feature | Standard model | Executive-focused model |
|---|---|---|
| Device access | Often highly restricted | Managed access may be allowed |
| Privacy | Shared space is common | Private rooms are more common |
| Census | Larger groups | Smaller population |
| Therapy mix | More group-heavy | More individual attention |
| Work accommodation | Usually limited | Designed around essential obligations |
That doesn't mean executive treatment is automatically better. It means it may fit better when career realities would otherwise prevent treatment.
What actually helps professionals stay in care
The structure that tends to matter most isn't the luxury language. It's the clinical intensity paired with discretion. According to Yellowstone Recovery's Costa Mesa rehab information, executive programs with a small census of 5 to 10 clients and a minimum of four individual therapy sessions weekly correlate with 40 to 60% higher long-term abstinence rates and can reduce treatment dropout by 35% among executives concerned about career disruption.
Those numbers point to something families can observe directly. Small programs can respond faster. Staff know when a client is withdrawing emotionally, destabilizing psychiatrically, or retreating into work. In a larger setting, that can get missed.
Look for these practical features:
- Small census so clients aren't lost in the shuffle.
- Private rooms or quiet accommodations that protect confidentiality and rest.
- Tech-friendly policy for essential communication, not endless screen time.
- High frequency of individual sessions instead of relying almost entirely on groups.
- Clinical staff who understand licensed and high-profile professions where disclosure has real consequences.
The right executive feature isn't the one that feels most exclusive. It's the one that removes the excuse that would otherwise keep the person from entering or completing treatment.
Programs that market executive care but can't describe how they manage privacy, devices, boundaries, and professional stress in a clinically sound way usually haven't thought thoroughly about this population.
How to Handle Insurance and Private Pay Options
A common call goes like this. A spouse or business partner has finally convinced someone to get help, the program says it “accepts insurance,” and everyone assumes the hard part is over. Then the estimate arrives, and the family learns that detox may be covered one way, residential another, and the privacy features that made treatment possible may be self-pay.
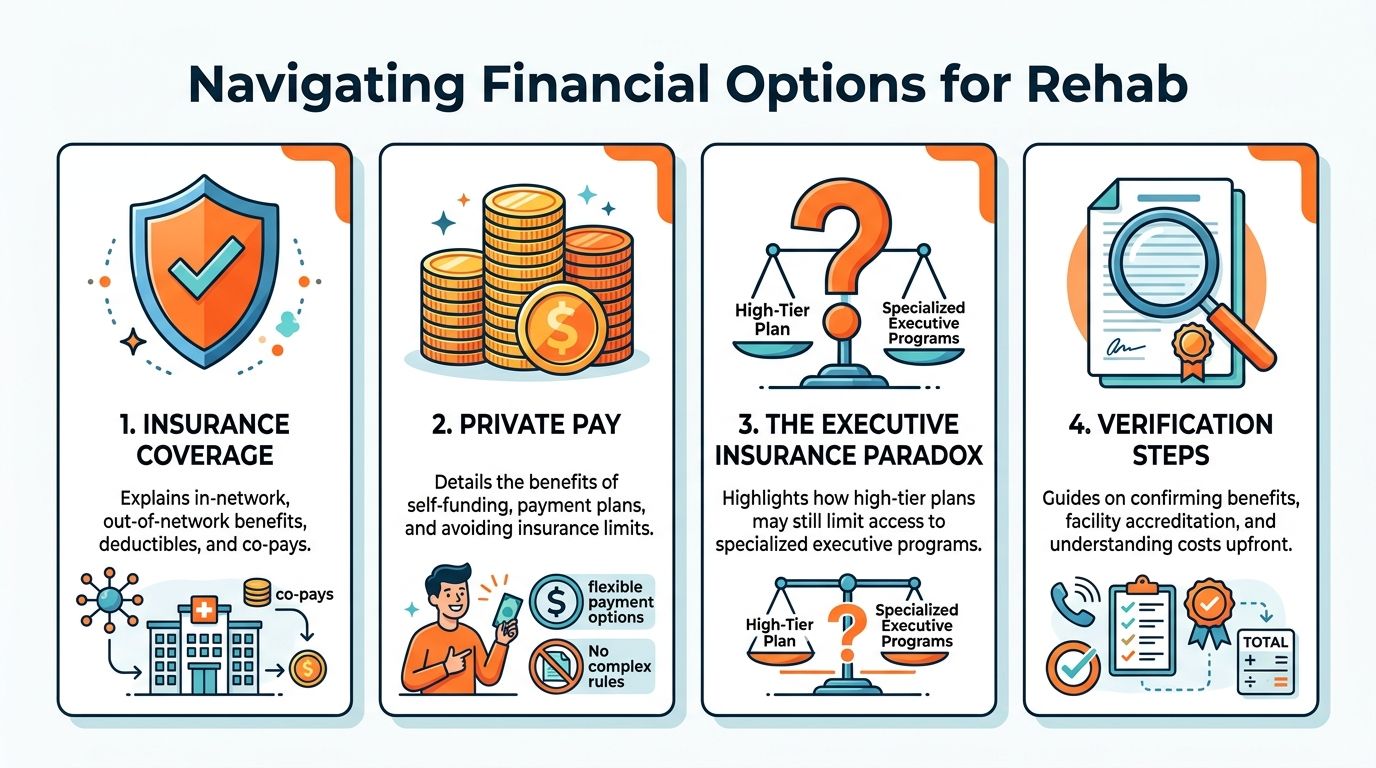
That gap between “we take your insurance” and “here is your real cost” causes more confusion than almost anything else in admissions. In Costa Mesa, pricing varies widely based on level of care, length of stay, medical complexity, room type, and whether executive accommodations are folded into the rate or billed separately. Families need line-item clarity, not general reassurance.
Why professionals often pay more than expected
The sticking point is rarely the core therapy itself. It is the added structure that lets a physician, attorney, founder, or senior executive step away from work without creating a second crisis.
American Addiction Centers' executive rehab guide explains that insurers often do not cover non-clinical features tied to executive programming, such as work-related conveniences or upgraded accommodations. A program can legitimately state it offers executive treatment and also legitimately state it accepts insurance. Those statements do not mean the executive-specific pieces are reimbursable.
That distinction matters for privacy too. Some professionals choose private pay because they want tighter control over who receives billing records, utilization reviews, and treatment updates. Insurance can reduce cost, but it usually adds review requirements, documentation demands, and the possibility that approved days change mid-stay.
Questions to ask before you agree to admission
Ask for a written verification of benefits and a written estimate. Verbal summaries are not enough.
Get answers to these questions:
Which level of care is being verified
Detox, residential, PHP, and IOP are often covered under different rules.Is the program in-network or out-of-network
That changes deductibles, coinsurance, reimbursement, and the risk of a larger balance bill.What services are billed as clinical care
Therapy, psychiatry, medication management, and nursing should be separated from room upgrades or work-access features.What is the estimated out-of-pocket range
Ask for the best-case and likely-case numbers based on current benefits.Who handles continued-stay reviews
If the insurer authorizes fewer days than the clinical team recommends, you need to know what happens next.What refunds or payment obligations apply if the plan changes
This matters if coverage is denied, reduced, or delayed after admission.
Ask the admissions team to split charges into two categories. What is billable medical treatment, and what is elective, privacy-related, or convenience-based self-pay.
When private pay can be the better choice
Private pay makes sense in some cases, especially for people whose careers depend on discretion, schedule control, and fewer insurance reviews. It can also make planning easier. The family knows the rate, the services included, and the financial exposure from day one.
The trade-off is simple. You may spend more upfront, but you may get clearer privacy protections, fewer coverage disputes, and more control over program design.
If a facility avoids written estimates, glosses over what insurance will not cover, or asks for a deposit before benefits are verified, reconsider the admission decision. Clear financial answers are part of good clinical process, not a separate sales conversation.
Red Flags to Spot When Choosing a Facility
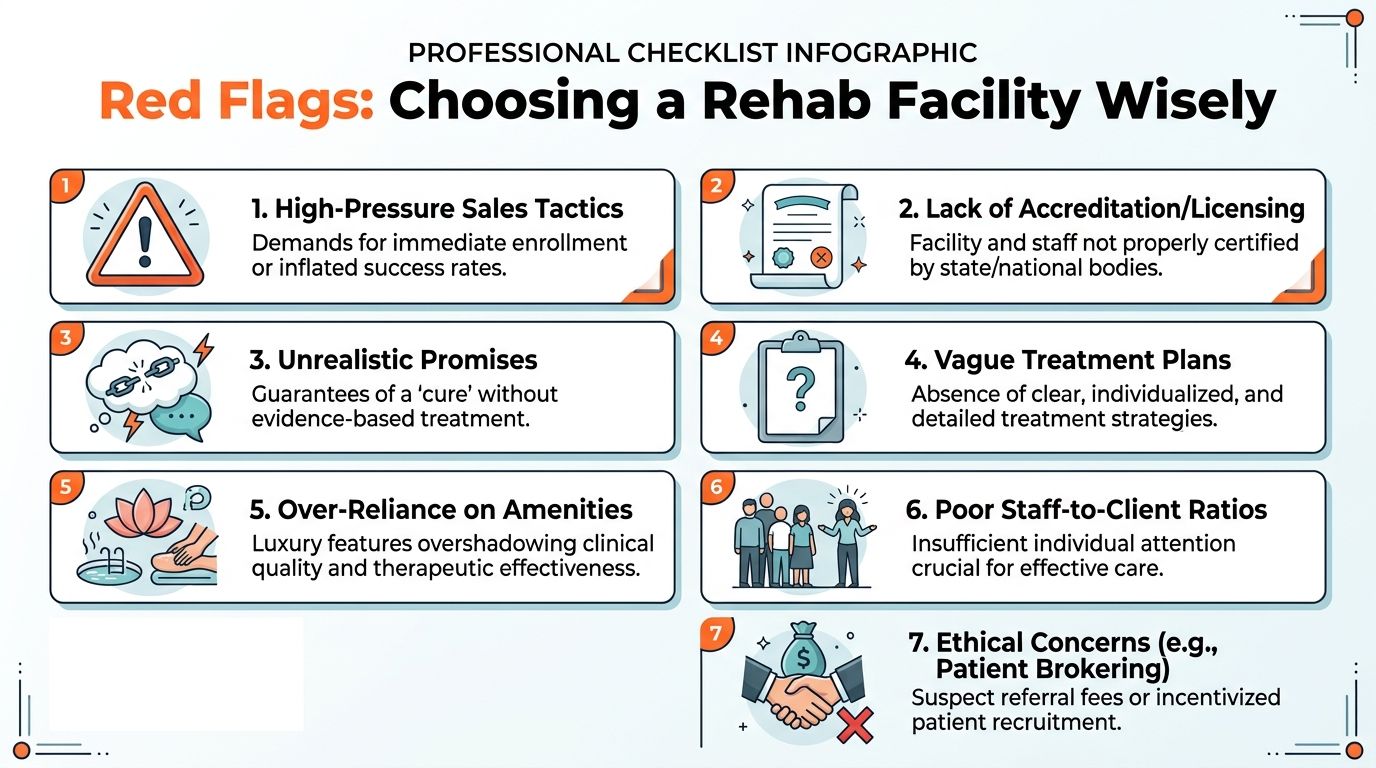
A common mistake happens on the first call. A spouse asks about detox, psychiatric care, work privacy, and cost. The admissions rep keeps steering the conversation back to a same-day bed, a beautiful house, and a deposit. That is not a small warning sign. It usually means sales is outrunning clinical judgment.
Costa Mesa has many treatment options, and that creates a real screening problem for families. Some programs are disciplined about assessment, staffing, and fit. Others are built to capture anxious callers quickly, especially people with strong insurance plans or the ability to private pay. For professionals and executives, the risk is higher. A poor fit can expose private information, interrupt work in unrealistic ways, or lead to a transfer after admission.
Signs that should slow you down
Watch for patterns like these during the first one or two conversations:
Pressure to commit before a real assessment
A legitimate program asks about substance use, mental health symptoms, medications, withdrawal risk, and prior treatment before talking about payment.Unclear answers about medical and psychiatric coverage
Ask who is physically on site, who is on call, and how psychiatric issues are handled after hours. Vague answers usually mean thinner coverage than the website suggests.No written explanation of privacy practices
Executives, physicians, attorneys, and public-facing professionals should ask how phones, laptops, employer contact, and record releases are managed. If the answer is improvised, privacy is not being handled carefully.Amenities carrying the whole pitch
Comfortable housing matters, but it does not treat alcohol withdrawal, stimulant relapse, trauma symptoms, or bipolar instability.A generic daily schedule
If every client gets the same template regardless of diagnosis, work obligations, or medication needs, expect a program built for occupancy rather than individualized care.Financial answers that stay verbal
If a facility will not put rates, likely out-of-pocket costs, and extra self-pay services in writing, families should be cautious.
Some red flags only show up when you ask harder questions.
Questions that expose weak programs
Who is not a fit for your program?
Strong facilities answer directly. They can tell you when someone needs a higher level of medical care, a different psychiatric setting, or a program with more structure.What happens if withdrawal or psychiatric symptoms worsen after admission?
Listen for a concrete protocol, not reassurance.How much individual clinical time is scheduled each week?
This helps separate true therapy-driven care from a model that relies mostly on groups.Who can access the patient's information, and how is employer communication handled?
Professionals need a precise answer here, especially when leave paperwork, licensing concerns, or reputation risk are in play.Can you send the treatment schedule, staffing model, and financial breakdown before admission?
A credible program should be able to do that without resistance.
A trustworthy facility gets more specific when the questions get harder.
Referral behavior also matters. Be careful if a caller seems eager to place your family member anywhere with an open bed, avoids naming ownership relationships, or deflects when asked why this program is a better fit than another one. In my experience, good admissions teams are willing to lose an admission if the clinical match is wrong. That protects the patient, and it often protects the family financially too.
Your Next Steps and a Recommended Local Option
If you're trying to choose the right Costa Mesa CA rehab, the most reliable path is to make the decision in this order.
First, confirm the level of care. A person detoxing from alcohol, benzodiazepines, or opioids may need medical detox before anything else. Second, confirm the clinical model. That means integrated treatment for substance use and mental health, not separate promises made by separate departments. Third, evaluate the fit for professional life. Privacy, limited census, and thoughtful technology policies can be the difference between entering treatment and postponing it again. Fourth, get a clear financial picture in writing before admission.
A short decision checklist
Use this when you're comparing calls with different programs:
Medical safety
Can they manage withdrawal appropriately and monitor complications?Psychiatric depth
Do they treat anxiety, depression, trauma, ADHD, or bipolar symptoms alongside addiction?Professional accommodations
Is there a realistic plan for privacy and essential work contact?Transparency
Can they explain programming, staffing, and costs without dodging specifics?
One Orange County option worth considering is Capo Canyon Recovery. It's located nearby in Mission Viejo and aligns closely with the standards that matter most for professionals and executives. The program offers detox and residential care with 24/7 nursing and psychiatric oversight, an executive treatment track, dual diagnosis treatment, a tech-friendly policy permitting cell phones and laptops, private bedrooms, and a small census of approximately five clients at a time. It also provides a minimum of four individual sessions weekly across disciplines, along with evidence-based therapies including CBT, DBT, ACT, EMDR, and Brainspotting. For families trying to balance confidentiality, clinical depth, and practical work realities, that combination is meaningful.
The right next step doesn't have to be a commitment to admission today. It can be a confidential call where you ask sharper questions and get honest answers. That alone moves the process forward.
If you want a discreet place to start, Capo Canyon Recovery offers confidential guidance for executives, professionals, and families who need medically supervised detox, residential treatment, dual diagnosis care, and a private setting that respects work and privacy concerns. A focused conversation with their team can help you clarify level of care, insurance options, and whether the program fits your situation before you make any decision.