The key difference is a single methyl group on methamphetamine, and that small change lets it cross the blood-brain barrier faster, producing a more potent, rapid, and neurotoxic effect than amphetamine. At an equivalent dose, methamphetamine releases approximately three to five times more dopamine than amphetamine, which is why the two drugs may sound related but behave very differently in the brain and in real life.
That gap gets missed all the time. Families hear that both are stimulants and assume the difference is mostly a matter of dose, street use, or branding. Clinically, that's not how it plays out. A tiny structural change creates a cascade of consequences, from stronger euphoria and faster addiction to radically different patterns of medical use, legal status, and treatment urgency.
If you're asking what is the difference between amphetamine and methamphetamine, the most useful answer isn't just chemical. It's practical. One substance appears commonly in legitimate medical treatment. The other is overwhelmingly associated with illicit production, far more destructive patterns of use, and a level of neurological risk that changes how I think about safety, monitoring, and recovery planning.
Amphetamine vs Methamphetamine An Introduction
Amphetamine and methamphetamine belong to the same stimulant family, but they are not interchangeable. The names are close enough to create confusion, especially for families trying to understand whether they're dealing with prescription misuse, illicit stimulant use, or a more serious escalation.
Here is the simplest clinical distinction: methamphetamine has one extra methyl group attached to the amphetamine structure. That single addition changes how quickly the drug enters the brain and how intensely it activates the reward system. The result is not a subtle variation. It is a different risk profile.
Early on, it helps to separate three questions:
- What is it chemically. Amphetamine and methamphetamine are closely related molecules, but methamphetamine is modified in a way that changes brain penetration.
- How is it used. Amphetamine commonly appears in regulated medications for ADHD and narcolepsy. Families often first encounter this issue through prescription stimulants such as those discussed in this overview of Adderall.
- Why does it matter clinically. Methamphetamine's faster and stronger effect tends to produce more destabilizing behavior, more severe crashes, and more urgent treatment needs.
Practical rule: If someone says, “They're basically the same drug,” that usually means they are overlooking the part that matters most, how fast, how hard, and how damaging the substance acts in the brain.
A concerned family member usually isn't asking for an organic chemistry lesson. They want to know whether the danger is meaningfully different. It is. That difference affects how quickly use can spiral, how long symptoms may persist, and how carefully a treatment team needs to assess mood, sleep, paranoia, cognition, and relapse risk.
The Critical Chemical and Pharmacological Divide
Why does one small chemical change lead to a much bigger clinical problem? Because the added methyl group on methamphetamine does more than alter a textbook structure. It changes how efficiently the drug gets into the brain, how strongly it drives reward signaling, and how hard it is for the person using it to regain control.
Methamphetamine is more lipid-soluble than amphetamine, which helps it cross the blood-brain barrier more readily, as described in this overview from the National Center for Biotechnology Information. In practice, that means a faster, sharper central nervous system effect. Families usually notice the result before they know the chemistry. More intensity. Less sleep. More agitation, impulsivity, and psychological destabilization.
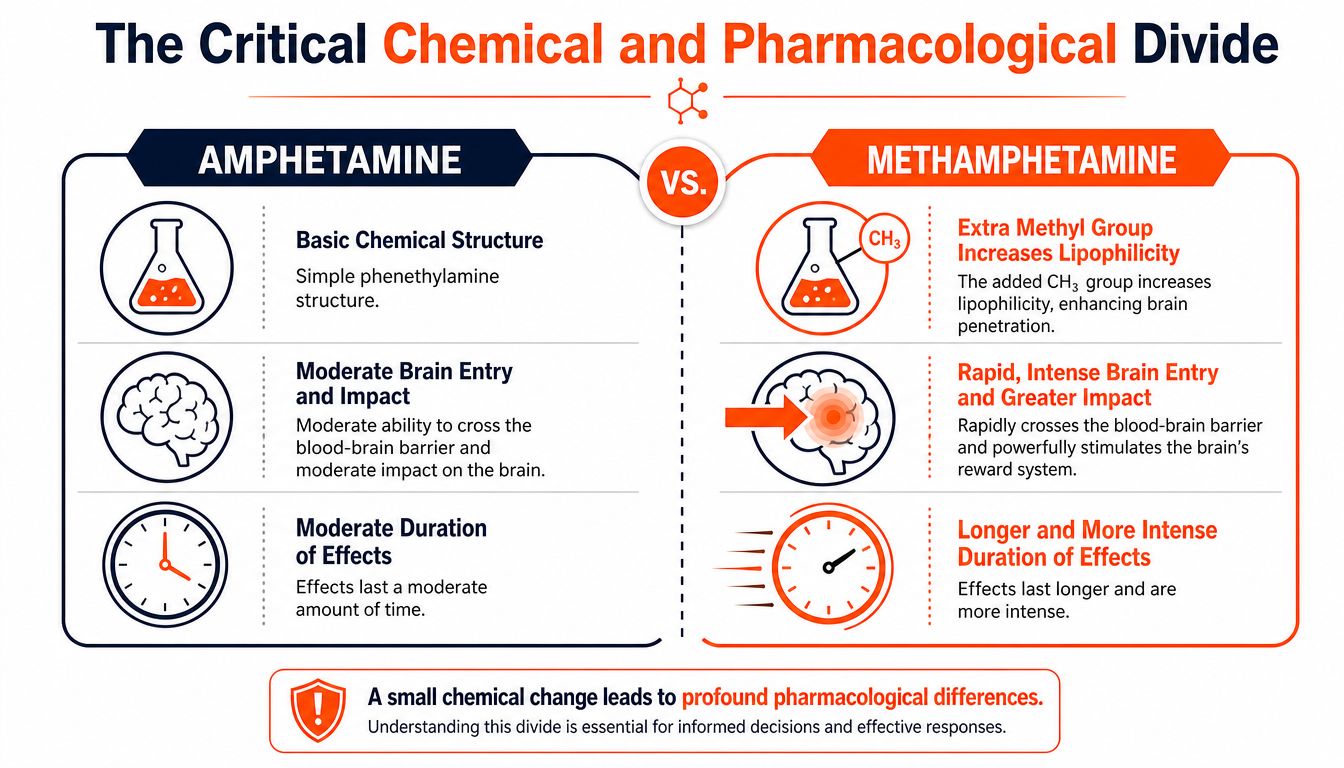
Why brain entry changes everything
A drug that reaches the brain faster usually feels more reinforcing. That matters in treatment because reinforcement shapes repetition, and repetition shapes addiction.
The National Institute on Drug Abuse explains that methamphetamine causes a rapid release of dopamine and other monoamines, producing a stronger rush and a higher risk pattern than related stimulants such as amphetamine, especially outside controlled medical use, as noted in this NIDA methamphetamine research report. Clinically, I see the downstream trade-off often. The same pharmacology that creates a more immediate effect also tends to create harsher crashes, longer periods of depletion, and more persistent craving.
That difference affects level-of-care decisions. A person using methamphetamine may need closer monitoring for paranoia, sleep deprivation, agitation, cardiovascular strain, and cognitive disruption than someone misusing a prescription amphetamine in lower amounts. For families evaluating options, a program built for methamphetamine addiction treatment should be prepared to assess those risks early and discreetly.
Why the same drug family can lead to different treatment needs
Amphetamine and methamphetamine both act on dopamine and norepinephrine systems, but they do not produce the same pattern of consequences in practice. Methamphetamine is more likely to be associated with compulsive binge use, prolonged wakefulness, suspiciousness, and stimulant-induced psychotic symptoms. Those are not minor differences. They change how a treatment team approaches detox support, psychiatric evaluation, relapse planning, and return to work.
This is also one reason legal status and prescribing patterns diverge so sharply, which the next section examines in more detail. The chemistry drives the pharmacology. The pharmacology drives behavior. Behavior drives medical, psychiatric, and legal fallout.
For professionals comparing stimulant medications in a legitimate medical setting, understanding ADHD drug choices can be helpful because it shows how small formulation and pharmacokinetic differences can produce very different patient experiences.
What clinicians look for
The useful question is not whether both substances belong to the stimulant family. The useful question is what pattern of use and impairment is present.
I look at route of administration, pace of escalation, days without sleep, appetite suppression, new paranoia, work impairment, and whether the person can stop without crashing into depression or agitation. Those details tell us far more than the label alone. They also help determine whether the person needs outpatient structure, a higher-acuity setting, or a confidential treatment plan designed for someone whose career cannot absorb public disruption.
Therapeutic Use Cases Versus Illicit Markets
The legal and medical divide between amphetamine and methamphetamine is sharp. That divide didn't happen by accident. It reflects how each drug performs in real-world practice and how much risk regulators, prescribers, and public health systems attach to each one.
Amphetamine has a recognized place in medicine. It is prescribed for conditions such as ADHD and narcolepsy in regulated formulations, with dose control, monitoring, and clear prescribing boundaries. By contrast, methamphetamine has almost no routine role in modern clinical care.
Where each substance shows up
According to this treatment overview comparing amphetamines and methamphetamine, globally, methamphetamine use affects an estimated 27 million users, while millions of children, adolescents, and adults regularly take prescription medications containing amphetamines for ADHD and narcolepsy. The same source notes that there is only one FDA-approved medication containing methamphetamine, Desoxyn®.
That single fact tells you a lot. Amphetamine is embedded in normal prescribing systems. Methamphetamine is not.
A second distinction matters just as much. The same source explains that almost all methamphetamine in the United States is manufactured illegally in clandestine labs, while amphetamine use involves both legally prescribed medications and illegally produced substances. Clinically, that means methamphetamine use often comes with additional uncertainty about purity, contamination, route of use, and binge patterns.
Why this changes the conversation with families
When families hear “stimulant,” they sometimes frame the issue as a misuse problem on a spectrum. Sometimes that's true. But if the substance is methamphetamine, the treatment conversation has to widen quickly.
- Medical context differs. Prescription amphetamines can be part of legitimate care when monitored appropriately.
- Supply chain risk differs. Illicit methamphetamine introduces unknowns that don't exist in standard pharmacy dispensing.
- Behavioral deterioration can be faster. By the time many families recognize the pattern, work performance, sleep, and judgment may already be significantly impaired.
People who are sorting out whether side effects are coming from a legitimate ADHD medication versus misuse may also benefit from insights into ADHD treatment side effects, especially when the question is whether a prescribed stimulant is causing problems or whether something more dangerous may be happening.
If methamphetamine use is part of the picture, the issue moves beyond medication management and into addiction medicine. Families often need a more direct understanding of meth addiction treatment options so they can stop treating the situation like a medication adjustment problem.
A prescription bottle and an illicit stimulant may both sit under the umbrella of “stimulants,” but they do not carry the same medical meaning, legal reality, or treatment implications.
Comparing Acute and Long-Term Health Effects
When families ask what is the difference between amphetamine and methamphetamine, this is often the section they need most. They don't just want chemistry. They want to know what each drug does to a person they love.
The short answer is that both can cause serious harm when misused, but methamphetamine usually presents as the more intense and more destabilizing substance, both immediately and over time.
Amphetamine vs. Methamphetamine A Clinical Comparison
| Attribute | Amphetamine (e.g., Adderall) | Methamphetamine (e.g., Crystal Meth) |
|---|---|---|
| Primary pattern | Often seen in prescription treatment and in misuse of those medications | Predominantly associated with illicit production and use |
| Brain effect | Stimulant effect with increased alertness, energy, and focus | More rapid, forceful stimulant effect with stronger reward activation |
| Acute presentation | Restlessness, reduced appetite, insomnia, anxiety, elevated heart rate and blood pressure | More intense euphoria, more severe agitation, prolonged sleeplessness, paranoia, stronger cardiovascular strain |
| Long-term concern | Dependence, mood disturbance, cardiovascular stress, cognitive and functional decline when misused | Direct neurotoxicity, psychosis risk, severe weight loss, dental destruction, cognitive impairment, broader physical deterioration |
| Treatment urgency | Can range from outpatient assessment to higher levels of care depending on misuse severity | More often requires close monitoring, structured detox, and intensive treatment planning |
This visual summary helps many readers organize the difference quickly.
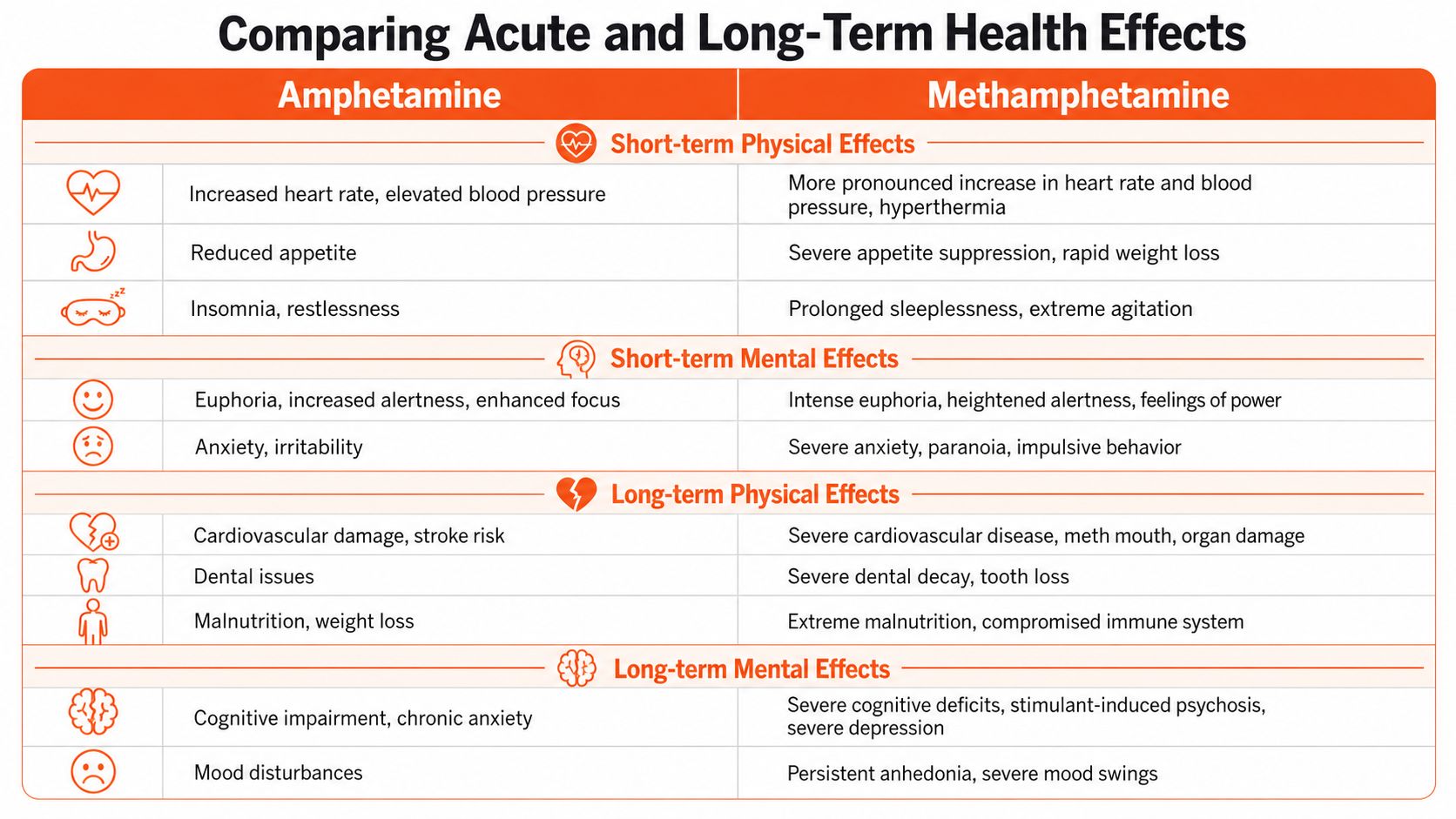
Short-term effects in the room
Both substances can raise heart rate, increase blood pressure, suppress appetite, disturb sleep, and produce anxiety or irritability. With methamphetamine, the same categories often appear in a more amplified form. A person may be awake longer, eat less, become more reactive, and move from confidence to agitation very quickly.
This matters in the clinic because the immediate risk assessment has to include not just intoxication, but also judgment, impulsivity, hydration, nutrition, and cardiovascular stress. For readers who want a broader overview of stimulant-related cardiac complications, this medical guide to drug-related heart issues is a useful reference.
Long-term consequences are not symmetrical
The verified data draw a hard line here. Methamphetamine is directly neurotoxic to dopamine and serotonin neurons at recreational doses, whereas amphetamine at therapeutic doses does not produce measurable brain damage in the same way, as noted earlier in the pharmacology source. That distinction matters because it changes expectations for mood, motivation, cognition, and recovery trajectory.
Common long-term patterns seen with methamphetamine use include:
- Severe physical depletion. Appetite suppression can become extreme, with visible weight loss and general deterioration.
- Dental destruction. Families often recognize “meth mouth” late, after substantial damage has already occurred.
- Psychiatric instability. Paranoia, suspiciousness, agitation, and stimulant-induced psychosis become more likely as sleep and nutrition collapse.
- Cognitive fallout. Attention, memory, planning, and emotional regulation often suffer.
Amphetamine misuse can still be serious. It can drive insomnia, anxiety, compulsive redosing, cardiovascular strain, and dependence. But in clinical practice, methamphetamine usually produces a broader pattern of damage across mood, behavior, physical appearance, and social functioning.
If a loved one is becoming physically gaunt, sleeping very little, acting suspicious, and deteriorating quickly, I would worry far more about methamphetamine than about straightforward prescription stimulant misuse.
Addiction Potential Withdrawal and Overdose
Why does one added methyl group matter so much here? Because that small chemical change does not stay small in the body. It changes how quickly the drug reaches the brain, how intensely it drives dopamine release, and how fast use can shift from occasional to compulsive. That is the clinical difference families and employers end up living with.
Methamphetamine often creates a steeper slide. In practice, I see people lose control faster, recover more slowly between episodes, and make riskier decisions while convinced they are still managing the situation. Amphetamine misuse can also become severe, especially when someone starts taking more than prescribed, crushing tablets, using medication that was not prescribed to them, or using stimulants to keep up with unrealistic demands. The timeline is usually less forgiving with methamphetamine.

Why methamphetamine often progresses faster
Researchers at the National Institute on Drug Abuse describe methamphetamine as a potent, highly addictive central nervous system stimulant, and that pattern fits what treatment programs see every day: faster reinforcement, more compulsive redosing, and a shorter distance between experimentation and a full use disorder. The same chemistry discussed earlier helps explain why. Methamphetamine reaches the brain efficiently and produces a stronger reward signal, so the brain learns the drug with unusual speed.
https://nida.nih.gov/publications/research-reports/methamphetamine/what-methamphetamine
Families rarely describe this in pharmacology terms. They describe a person who stops sleeping normally, starts missing meals, becomes irritable or secretive, overpromises, crashes, and then uses again to function. For professionals, this can stay hidden longer because performance may hold on in public after judgment has started to erode in private.
Withdrawal is more than fatigue
Stimulant withdrawal is often underestimated because it does not usually look like alcohol or sedative withdrawal. The medical risk is often lower. The psychiatric risk can be serious.
Both drugs can produce exhaustion, depression, irritability, poor concentration, sleep disruption, and cravings. Methamphetamine withdrawal often brings a deeper crash, a flatter mood, and a more prolonged inability to feel normal reward. That matters in treatment because the person may not present as dramatic. They may present as hopeless, shut down, impulsive, or ready to use again just to make the crash stop.
If prescription stimulant misuse is part of the picture, it helps to understand how long Adderall withdrawal can last and when symptoms need clinical supervision.
For physicians, executives, attorneys, pilots, and other professionals, withdrawal also carries a practical threat. Shame keeps people isolated. Isolation increases relapse risk. Discreet treatment works best when it addresses sleep, mood, cravings, work impairment, and the fear of professional exposure at the same time.
Overdose risk follows a different pattern
Both substances can lead to overdose or other medical emergencies. With amphetamine, that risk often rises when someone takes far above the prescribed dose, redoses repeatedly, or mixes stimulants with alcohol, benzodiazepines, cocaine, or other substances.
Methamphetamine adds more unpredictability. Illicit supply is inconsistent. Purity varies. Contaminants are common. People may also stay awake for days, become dehydrated, stop eating, develop paranoia, or keep using long after their body is showing clear signs of strain. In practice, overdose is not always a simple collapse. It may look like chest pain, severe agitation, dangerous overheating, hallucinations, panic, violent blood pressure elevation, or psychosis.
That is why I tell families to stop debating whether the person is "just tired" or "coming down." If someone is acutely agitated, severely sleep deprived, paranoid, chest-pain positive, confused, or talking about hopelessness, they need immediate medical evaluation and close monitoring. Reassurance alone is not a treatment plan.
When Professional Treatment Becomes Necessary
Families usually ask for help after trying everything else first. They've had the hard conversations. They've covered for missed responsibilities. They've accepted explanations that no longer make sense. By the time treatment is on the table, the issue often isn't whether help is needed. It's whether help will be specific enough, private enough, and medically sound enough.
That matters even more with stimulant problems because the person may still be functioning in public while deteriorating in private. Executives, physicians, attorneys, pilots, first responders, and business owners often keep working long after their sleep, judgment, and emotional stability have started to break down.

Signs the situation has crossed into treatment territory
Watch for patterns, not isolated incidents.
- Escalating loss of control. They keep promising to stop, cut back, or use only in certain situations, and they can't hold that line.
- Functional decline behind the scenes. Work may still look intact, but sleep, finances, relationships, or judgment are slipping.
- Psychiatric red flags. Paranoia, panic, severe depression, suspiciousness, or stimulant-related psychotic symptoms require immediate attention.
- Physical instability. Extended wakefulness, dramatic appetite loss, chest symptoms, dehydration, or visible deterioration call for medical oversight.
- Dual diagnosis clues. Anxiety, burnout, trauma, ADHD, or depression may be fueling the substance use and need concurrent treatment.
What good treatment actually includes
For stimulant use, detox is less about a single withdrawal protocol and more about stabilization. The team has to manage sleep recovery, nutritional deficits, mood changes, cravings, medication review, and safety. Continuous nursing and psychiatric oversight are important when someone is agitated, severely depressed, or cycling between exhaustion and activation.
Residential treatment becomes necessary when the person needs separation from access, daily structure, intensive therapy, and integrated care for co-occurring conditions. In my experience, this is especially important for professionals who have learned to compensate outwardly while fragmenting internally.
A high-functioning person often needs:
- Privacy that reduces reputational fear
- A setting small enough for individualized attention
- Psychiatric care that can sort out ADHD, anxiety, depression, trauma, and burnout from substance effects
- Enough flexibility to remain connected to critical responsibilities without letting work become an escape from treatment
Treatment works better when it addresses the reason the stimulant became necessary to the person, not just the fact that they used it.
Discreet, specialized care is often the difference between delayed help and accepted help. Professionals are more likely to engage when treatment protects confidentiality, allows thoughtful communication with essential work contacts, and treats substance use and mental health as one clinical picture instead of two separate problems.
If you or someone you care about is dealing with amphetamine misuse, methamphetamine use, or the fallout that often comes with stimulant addiction, Capo Canyon Recovery offers medically supervised detox and private residential treatment designed for professionals who need real clinical care without sacrificing privacy. The program combines 24/7 nursing, psychiatric support, dual diagnosis treatment, private rooms, and a tech-friendly environment that allows essential work communication while recovery takes priority.